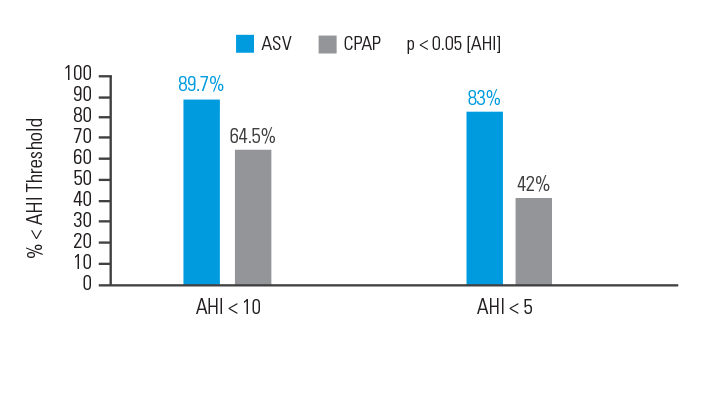
In an intention-to-treat analysis, success (apnoea hypopnoea index [AHI] < 10) at 90 days of therapy was achieved in 89.7% of patients treated with ASV versus 64.5% of participants treated with CPAP.6
[N = 66, prospective randomised trial]
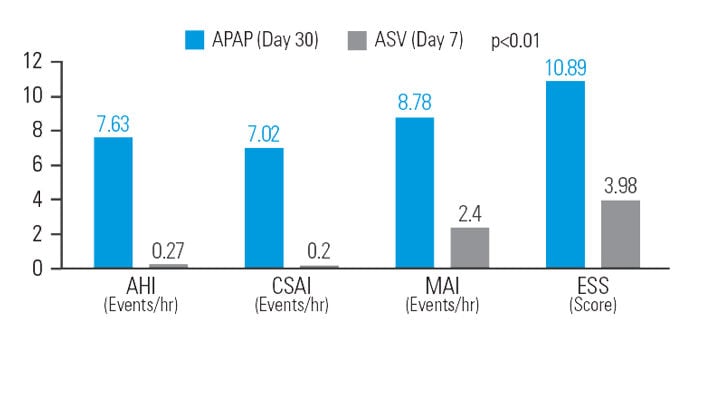
After 30 days of APAP treatment, ASV provided a further reduction (compared to baseline) of 12.9% in AHI, 48.5% in central sleep apnoea index (CSAI), 26.1% in micro-arousal index (MAI), and 37.9% in Epworth Sleepiness Scale (ESS) score at similar mean pressure.7
[N = 42, sequential study]
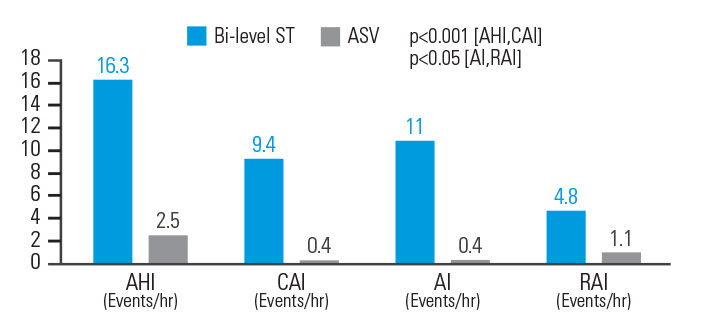
In opioid-induced CSA, ASV therapy reduced AHI by 84.7%, central apnoea index (CAI) by 95.7%, Apnoea Index (AI) by 96.4%, and respiratory arousal index (RAI) by 77.1% when compared to bi-level ST. Respiratory parameters were normalised in 83.3% of patients on ASVAuto but only 33.3% of patients on bi-level ST.8
[N = 18, prospective, randomised crossover polysomnography study]
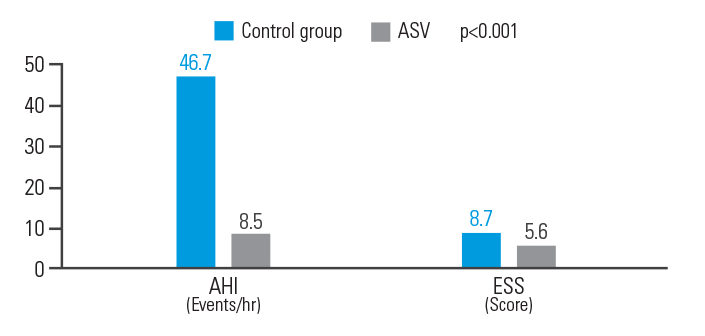
ASV therapy improved outcomes for post-acute ischemic stroke patients with CSA, reducing AHI by 81.8% and ESS by 35.6%.9
[N = 15, single centre retrospective analysis]