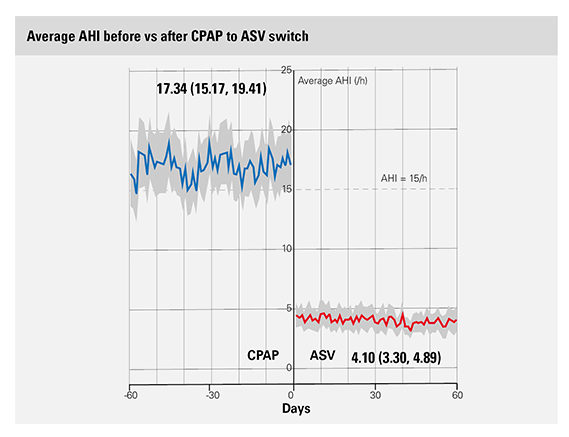
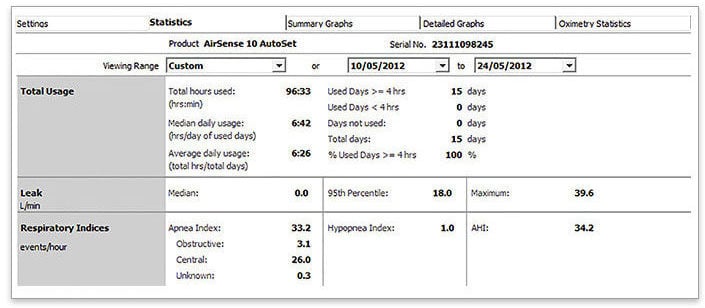
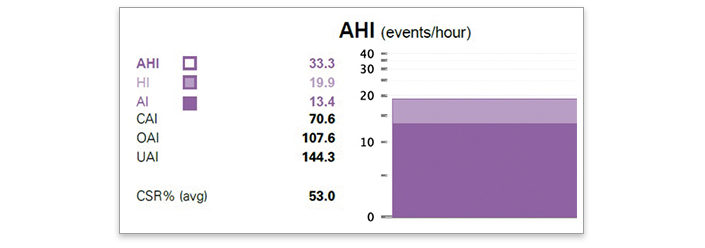
The average AHI before the CPAP to ASV switch among patients with emergent or persistent CSA was 17.34/hour as compared with 4.1/hour after the switch.
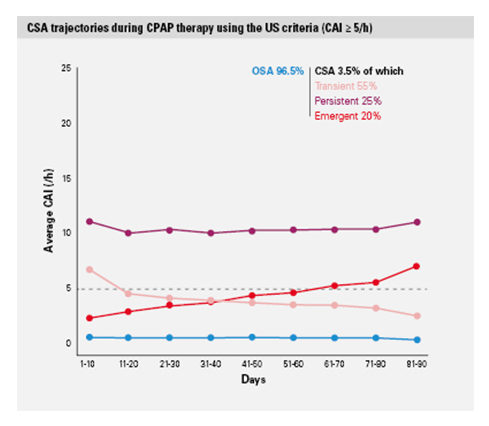
The data suggest that if CSA persists after 2 weeks, the patient fits within the trajectory of emergent or persistent CSA and may benefit from a switch to ASV.*
The study was led by an external international committee of sleep and respiratory experts: Jean-Louis Pépin (France), Holger Woehrle (Germany), Atul Malhotra (USA), and Peter Cistulli (Australia).