A bilevel PAP device with adaptive pressure support designed to stabilise breathing and personalise therapy for patients with central sleep apnea, obstructive sleep apnea, mixed apneas or periodic breathing.




Featuring a seamlessly integrated connected care system with enhanced support features and over-the-air updates, AirCurve 11 ASV* delivers a responsive adaptive servo-ventilation (ASV) algorithm.
It is designed to stabilise breathing2 in patients with central or mixed sleep apnea, or who have periodic breathing with or without obstructive events.
*ASV therapy is contraindicated in patients with chronic, symptomatic heart failure (NYHA 2-4) with reduced left ventricular ejection fraction (LVEF ≤ 45%) and moderate to severe predominant central sleep apnea.

Standard therapies are often unable to fully normalise breathing for patients with pauses in breathing due to the absence of respiratory effort. AirCurve 11 ASV offers a simple solution to complex needs by combining the trusted algorithms of AirCurve™ 10 with Resmed Air11™ connected features. Offering a straightforward setup, the AirCurve 11 ASV’s algorithm has only four clinical settings. It comes with two modes: ASV with fixed EPAP and ASVAuto, which automatically adjusts the EPAP.

Leveraging Breath Phase Mapping technology, the ASV algorithm dynamically adjusts inspiratory pressure support on a breath-by-breath basis in response to reductions in ventilation to help maintain ventilation near a target level. As breathing stabilises, pressure support gradually reduces toward a comfortable minimum level, helping mitigate hyperventilation and associated hypocapnia.
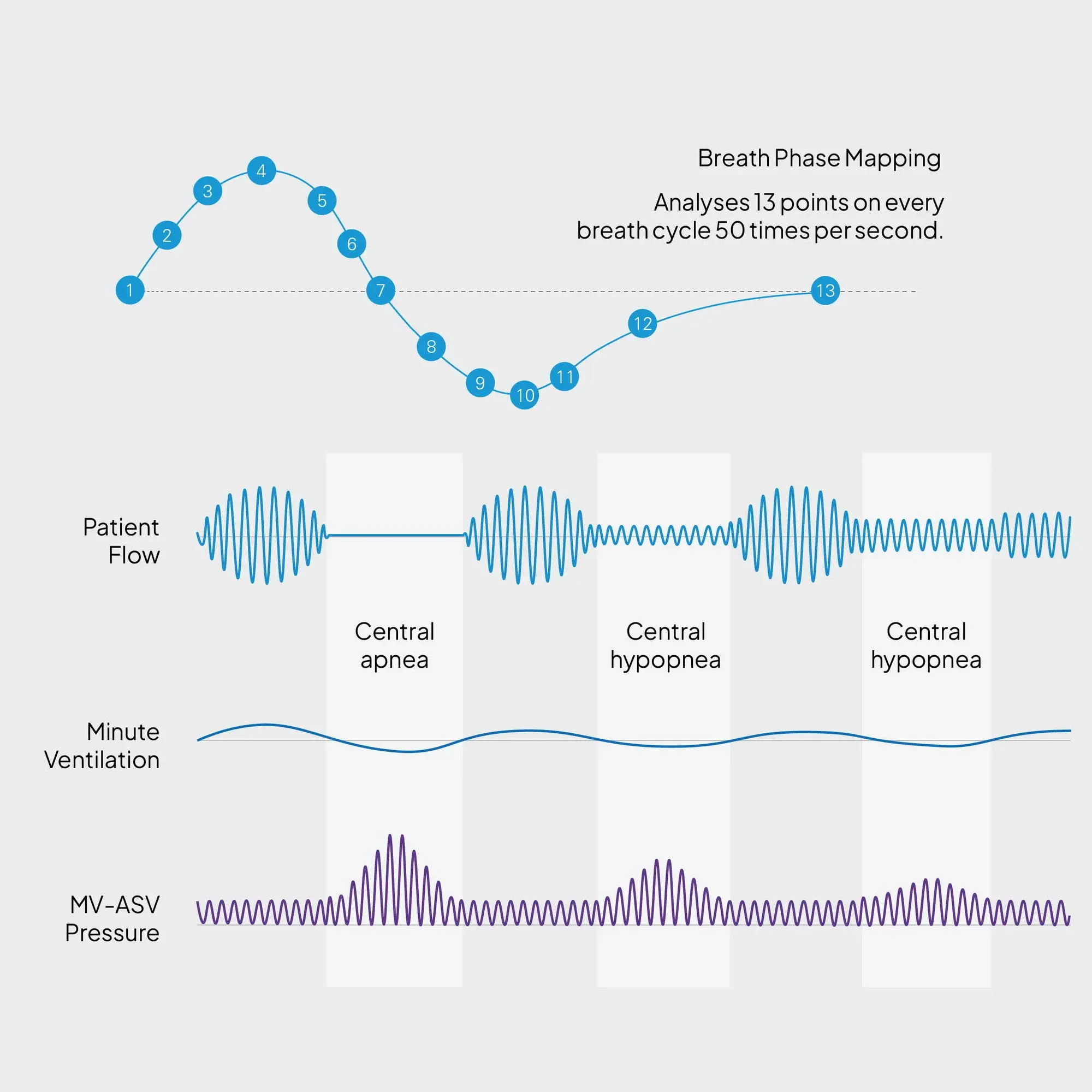
Designed to counterbalance ventilatory instability, pressure support (PS) auto-adjusts between the Min PS and the Max PS to maintain each patient’s unique minute ventilation target (tidal volume and respiratory rate) while maintaining patient-device synchrony and comfort.
Auto-adjusts expiratory positive airway pressure (EPAP) within the allowed range (Min EPAP and Max EPAP) to maintain upper airway patency.
Uses breath phase mapping to provide a timed backup rate synchronised with the patient’s own breathing to maintain the target minute ventilation in the case of apneas.
CAI ≥ 5/h in week 1, < 5/h in week 13
CAI ≥ 5/h in week 1, ≥ 5/h in week 13
CAI < 5/h in week 1, ≥ 5/h in week 13
